China's First Estrogen Receptor 1 (ESR1) Inhibitor Indicated for Breast Cancer Obtains Marketing Authorization
On June 22, 2026, the National Medical Products Administration of China officially granted marketing approval to LLY's Class 1 innovative drug Imlunestrant ( INLURIYO). This drug has two approved indications: ① As monotherapy, it is indicated for the treatment of adult patients with locally advanced or metastatic breast cancer that is estrogen receptor (ER)-positive, human epidermal growth factor receptor 2 (HER2)-negative, and harbors estrogen receptor 1 (ESR1) mutations, who have received prior endocrine therapy; ② In combination with abemaciclib, it is indicated for the treatment of adult patients with locally advanced or metastatic breast cancer that is ER-positive, HER2-negative, and harbors ESR1 mutations, who have received prior endocrine therapy. The marketing approval of this drug provides a new treatment option for breast cancer patients with endocrine therapy resistance and ESR1 gene mutations.
PART 1
Basis for Approval
This approval is primarily grounded in the positive outcomes of the global multicenter, randomized controlled phase III EMBER-3 clinical trial (NCT04975308)[1]. The trial enrolled 874 adult patients diagnosed with estrogen receptor-positive (ER+)/human epidermal growth factor receptor 2-negative (HER2-) advanced breast cancer, who had previously received treatment with aromatase inhibitors, with or without CDK4/6 inhibitors, and had not undergone chemotherapy. Eligible participants were randomized into three arms at a 1:1:1 allocation ratio: the imlunestrant monotherapy arm (n=331), the standard-of-care arm (fulvestrant or exemestane, n=330), and the combination therapy arm (imlunestrant plus abemaciclib, n=213).
The primary endpoints of the trial were: (1) progression-free survival (PFS) comparing imlunestrant monotherapy versus standard-of-care in patients harboring estrogen receptor 1 (ESR1) gene mutations; and (2) PFS comparing the combination therapy versus imlunestrant monotherapy in the overall trial population. The secondary endpoints included overall survival (OS) corresponding to the comparisons specified in the primary endpoints. As of the data cut-off in August 2025, the median follow-up duration across the trial cohort was 28.5 months.
Among patients with ESR1 gene mutations, the median PFS (mPFS) of the imlunestrant monotherapy arm was 5.5 months, which was superior to the 3.8 months observed in the standard-of-care arm, representing a 38% reduction in the risk of progression or death (hazard ratio [HR]=0.62, 95% confidence interval [CI]: 0.47-0.82, P=0.0007). The median OS (mOS) in the imlunestrant monotherapy arm reached 34.5 months, which was significantly better than the 23.1 months in the standard-of-care arm, corresponding to a 40% reduction in the risk of death (HR=0.60, 95% CI: 0.43-0.86, P=0.0043) (Figure 1, Figure 2).
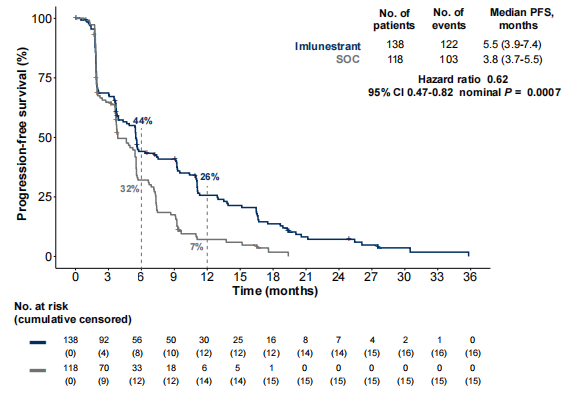
▲Figure1 mPFS in patients with ESR1 mutation
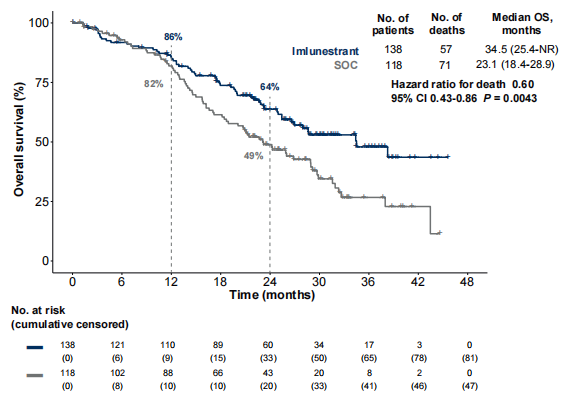
▲Figure2 mOS in patients with ESR1 mutation
Across the entire patient cohort, the median progression-free survival (mPFS) in the combination therapy (Imlunestrant plus Abemaciclib) group was 10.9 months, representing a clinically meaningful improvement over the 5.5 months observed in the Imlunestrant monotherapy group. The combination therapy reduced the risk of death or progression by 41% (hazard ratio [HR] = 0.59, 95% confidence interval [CI]: 0.47–0.74, P ≤ 0.0001). At the time of data cutoff, the median overall survival (mOS) had not been reached in the combination therapy (Imlunestrant plus Abemaciclib) group, while the mOS of the Imlunestrant monotherapy group was recorded as 34.4 months (Figure 3, Figure 4).
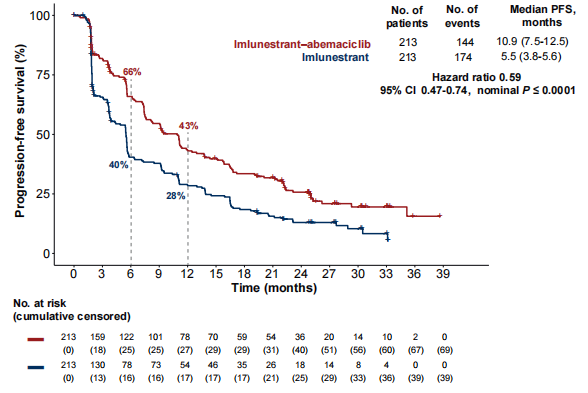
▲Figure3 mPFS for all patient populations in Figure 3
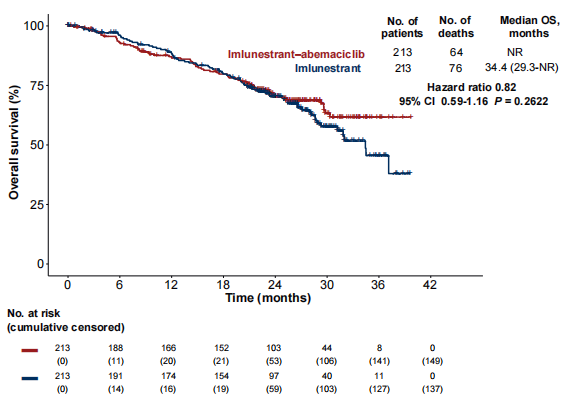
▲Figure4 All patient populations mOS
PART2
ESR1 Gene and Endocrine Therapy Resistance
Breast cancer ranks first globally among all cancer types in terms of new incidence and mortality among women. It is also highly prevalent among Chinese women, with its incidence second only to that of lung cancer. Among all breast cancer cases, the ER+/HER2- subtype accounts for approximately 70%, and endocrine therapy serves as a critical cornerstone of treatment for patients diagnosed with this subtype. Nevertheless, 20% to 40% of patients who have previously received endocrine therapy, particularly aromatase inhibitors, develop endocrine therapy resistance[2].
Existing studies have demonstrated that ESR1 gene mutations represent a key mechanism underlying acquired endocrine therapy resistance in patients with ER+/HER2- breast cancer. ESR1 gene mutations induce constitutive activation of the encoded ER protein, enabling the ER signaling pathway to continue driving hormone-dependent cell transcription and proliferation in the absence of ligands (estrogen), thereby evading the inhibitory effect of endocrine therapeutic drugs[3]. To date, more than 50 ESR1 site mutations have been identified, most of which occur in the ER ligand binding domain (AF-2/LBD). Common mutation sites include D538G (33%), Y537S (18%), and E380Q (13%), and the ESR1 gene may exhibit the phenomenon of co-mutation at two or more sites (Figure 5)[4].
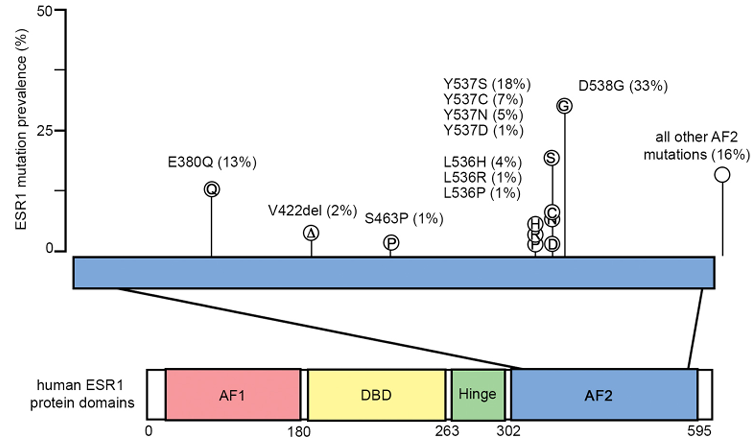
▲Figure5 ESR1 gene mutation site
PART3
ESR1 gene mutation detection
According to the *CSCO Guidelines for the Diagnosis and Treatment of Breast Cancer (2026 Edition)*, for patients diagnosed with ER+/HER2- metastatic breast cancer who experience relapse or disease progression following endocrine therapy combined with CDK4/6 inhibitors, routine ESR1 gene mutation testing is recommended. Given that ESR1 mutations are typically acquired mutations, re-testing of tissue or liquid biopsy samples is required upon disease progression even if no mutation was detected in the initial test. Currently, the primary detection technologies for this purpose are next-generation sequencing (NGS) and polymerase chain reaction (PCR)[5].
The *NCCN Guidelines for Aggressive Breast Cancer, Version 4.2026* recommends that ESR1 gene mutation testing should be performed when disease progression occurs after completion of a prior endocrine therapy regimen, with blood testing as the preferred approach. If the initial ESR1 test returns a negative result, re-analysis of tissue samples using NGS technology is recommended (Figure 6)[6].
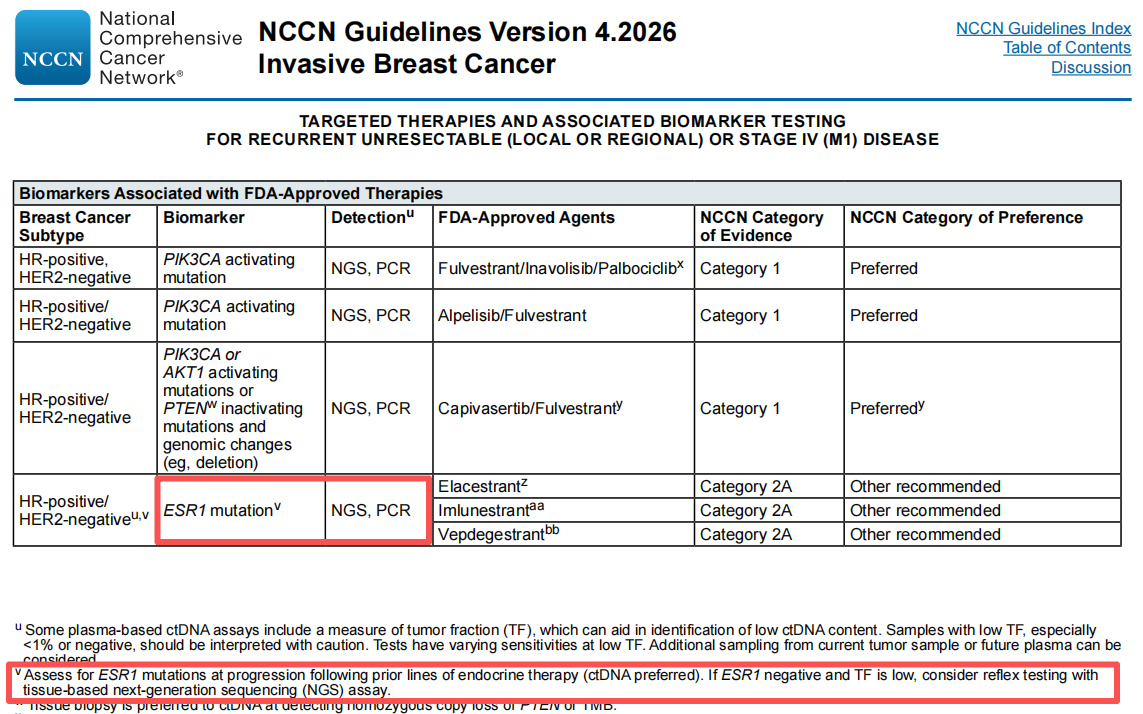
▲Figure6 NCCN breast cancer Diagnosis and Treatment guide
Utilizing the PAP-ARMS multiplex fluorescence PCR technique?, SpaceGen has developed the *Breast Cancer ESR1 Gene Mutation Detection Kit* (Figure 7). This product detects 11 mutations of the ESR1 gene in blood samples collected from breast cancer patients, covering common mutation hotspots including D538G, Y537S, and E380Q. It achieves a detection sensitivity as high as 0.2%, which substantially enhances the accuracy and specificity of detection, eliminates missed detection caused by insufficient detection sensitivity, and delivers reliable testing services for breast cancer patients with endocrine therapy resistance.
Meanwhile, this product adopts PCR detection technology recommended by both domestic and international clinical guidelines. It features a simplified operating workflow and a shortened detection cycle, making it the preferred option for initial etiological assessment of drug resistance among breast cancer patients with endocrine therapy resistance, particularly those resistant to aromatase inhibitors. Test results can be obtained more rapidly to inform the selection of subsequent treatment regimens.

▲Figure7 SpaceGen-Breast Cancer ESR1 Gene Mutations Detection Kit
PART4
Summary
The approval of imlunestrant has addressed the long-standing clinical gap in China for the treatment of endocrine drug-resistant breast cancer driven by ESR1 mutations. Notably, its combination therapy regimen with abemaciclib is the first therapy class to receive regulatory approval in the Chinese market ahead of all other global markets, demonstrating the "China speed" in facilitating patient access to innovative pharmaceutical products. With the commercial launch of imlunestrant, a novel precision treatment modality characterized by high efficacy, favorable safety profile and convenient administration will become available to the large cohort of patients with ESR1-mutant breast cancer in China.
Imlunestrant received FDA approval in September 2025 for the treatment of adult patients with advanced or metastatic ER-positive/HER2-negative breast cancer harboring ESR1 mutations, who have experienced disease progression following at least one line of prior endocrine therapy. Additionally, the FDA granted approval to elacestrant in January 2023 for the treatment of postmenopausal women and adult men with advanced or metastatic ER-positive/HER2-negative breast cancer harboring ESR1 mutations. To date, elacestrant has not received marketing approval in China. It is expected that with the accumulation of additional positive clinical evidence and the advancement of clinical research, an expanding range of therapeutic agents will become available to improve outcomes for breast cancer patients.
References
[1] Ann Oncol. 2026 Apr;37(4):532-543.
[2] Journal of Clinical Oncology,2010,28(3):509-518.
[3] Annual review of medicine,2011,62(1):233-247.
[4] Biochimica et Biophysica Acta (BBA)-Reviews on Cancer,2023,1878(1):188830.
[5] CSCO Breast Cancer Diagnosis and Treatment Guide (2026 Edition)
[6] Invasive Breast Cancer NCCN Guidelines Version 4.2026
Disclaimer: This article is intended for informational sharing purposes only. Should any issue concerning copyright or other related rights arise, please contact us promptly, and we will implement corrective measures without delay. We appreciate your cooperation.


 閩公網(wǎng)安備35021202000745
閩公網(wǎng)安備35021202000745